Adrenal Tumor Removal Hypokalemia
Can the removal of an adrenal tumor lead to hypokalemia?
# Post-Adrenalectomy Potassium Dynamics in Primary Aldosteronism
## Clinical Evidence & Efficacy
The short answer is **no** — adrenalectomy for unilateral primary aldosteronism (PA) typically **corrects** hypokalemia, not causes it. However, the postoperative period involves complex potassium shifts that require careful management.
### Correction of Hypokalemia
Multiple guidelines consistently demonstrate that adrenalectomy resolves hypokalemia in the vast majority of cases:
- **Biochemical cure rate**: A multicenter international study demonstrated a **94% biochemical cure rate** after adrenalectomy for unilateral PA [7].
- **Hypokalemia resolution**: Surgery corrects hypokalemia, improves hypertension control, and reduces antihypertensive medication burden; approximately **40% of cases achieve complete hypertension resolution** [2].
- **Clinical success**: Less than **20% of patients** require the same or higher doses of antihypertensive medication postoperatively [5][6].
### The Actual Postoperative Risk: Hyperkalemia
The predominant electrolyte disturbance after adrenalectomy is **hyperkalemia**, not hypokalemia. This occurs due to **rebound hypoaldosteronism** from chronic suppression of the contralateral adrenal gland.
**Incidence data**:
- **Japan**: Post-adrenalectomy hyperkalemia prevalence of **9.9%** [7]
- **Korea**: **3.3% transient** and **7.7% persistent** hyperkalemia [7]
- **Severe hyperkalemia**: Occurs in approximately **5% of PA cases**, more frequent with prolonged contralateral hypoaldosteronism [2]
**Risk factors for postoperative hyperkalemia** [7]:
- Elderly age
- Low preoperative eGFR
- Suppressed aldosterone secretion on the non-dominant adrenal side
## Perioperative Management Protocol
### Immediate Postoperative Period (Day 0–3)
| Parameter | Recommendation | Source |
|-----------|---------------|--------|
| **Mineralocorticoid receptor antagonists (MRAs)** | Discontinue on postoperative day 1 | [2][3][4] |
| **Potassium supplementation** | Withdraw unless serum K⁺ < 3.0 mmol/L | [2][3][4] |
| **IV fluids** | Use normal saline **without** potassium chloride; avoid/minimize isotonic saline in first 2–3 days | [2][3] |
| **Antihypertensives** | Reduce appropriately with frequent BP monitoring | [4] |
### Monitoring Schedule
- **Postoperative day 1**: Measure plasma aldosterone concentration (PAC), plasma renin activity (PRA) or direct renin concentration (DRC), serum potassium, and serum creatinine [2][3][4]
- **Days 3–5**: Repeat serum potassium measurement [2]
- **First weeks**: High sodium and fluid intake recommended to prevent hyperkalemia from rebound hypoaldosteronism [2]
### When Hypokalemia May Persist
The only scenario where hypokalemia might persist postoperatively is when potassium levels are **very low (<3.0 mmol/L)** — in such cases, cautious potassium replacement may continue [4]. However, this represents inadequate preoperative correction rather than surgery-induced hypokalemia.
**The following flowchart illustrates the standardized follow-up protocol for PA after adrenalectomy:**
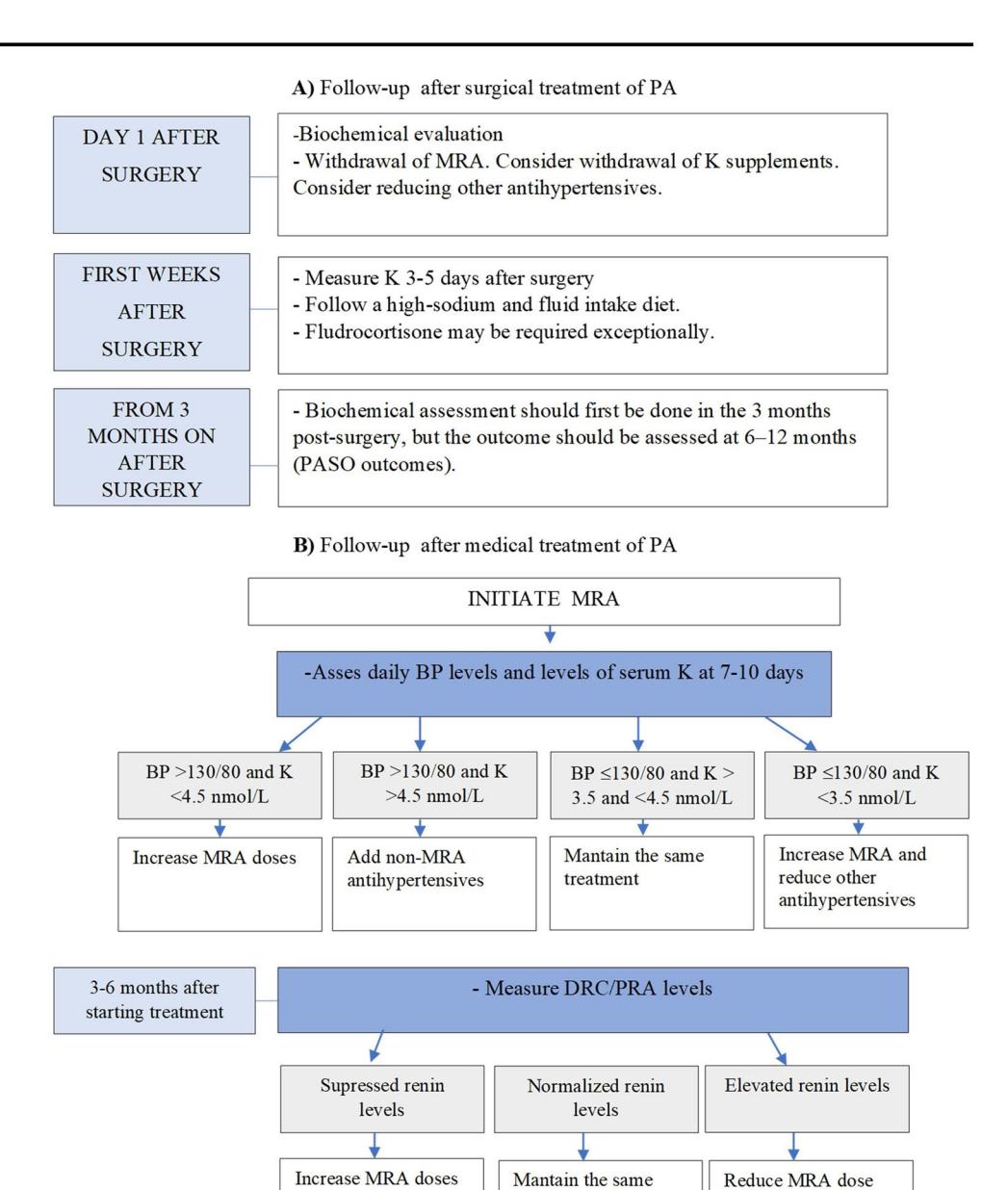
*Figure: Clinical flowchart outlining standardized follow-up protocols for Primary Aldosteronism following surgical adrenalectomy, including monitoring of biochemical response, blood pressure, and electrolyte management*
## Guideline Recommendations
| Organization | Key Recommendation | Grade |
|-------------|-------------------|-------|
| Japan Endocrine Society (2021) | Monitor serum potassium and renal function carefully post-adrenalectomy; hyperkalemia and decreased eGFR are frequent early findings | **1B** [7] |
| Korean Endocrine Society (2023) | Discontinue MRAs and potassium supplements on postoperative day 1; use normal saline without KCl unless K⁺ < 3.0 mmol/L | Guideline [3] |
| Taiwan Society of Aldosteronism | Discontinue potassium replacement and spironolactone immediately after adrenalectomy unless K⁺ < 3.0 mmol/L | Consensus [4] |
| AACE (2023) | Post-surgical follow-up should include biochemical assessment and individualized management | Consensus [1] |
## Critical Gaps
The current evidence does not provide:
- **Standardized criteria** for when to definitively judge biochemical cure after adrenalectomy (PAC typically decreases significantly within ~1 week, but renin suppression recovery may take >1 month) [7]
- **Long-term follow-up protocols** for patients with persistent hyperkalemia requiring fludrocortisone therapy
## Conclusion
Adrenalectomy for unilateral PA **corrects** pre-existing hypokalemia and carries a **94% biochemical cure rate**; the clinically significant postoperative electrolyte risk is **hyperkalemia** from contralateral adrenal suppression, occurring in 5–10% of cases, necessitating MRA discontinuation, potassium withdrawal, and careful electrolyte monitoring.
---
*This response is AI-generated based on retrieved clinical guidelines and literature. It is intended for clinical reference only. Clinicians should verify recommendations against local protocols and apply individual patient judgment in perioperative management.*