Acute Myocardial Infarction Introduction
Write a paragraph introducing acute myocardial infarction and acute heart failure for the introduction of a research paper.
## Acute Myocardial Infarction and Acute Heart Failure
Acute myocardial infarction (AMI) remains a leading cause of morbidity and mortality worldwide, accounting for 10–25% of all deaths in developed countries [11]. AMI results from prolonged myocardial ischemia, most commonly due to acute thrombotic occlusion of an atherosclerotic coronary artery following plaque rupture or erosion [4][9][10]. The ischemic insult triggers a cascade of cellular events—including glycogen depletion within 5 minutes, mitochondrial swelling by 20–30 minutes, and eventual irreversible necrosis—that culminates in the loss of functional myocardium [11][12]. Clinically, patients typically present with severe, crushing substernal chest pain that may radiate to the left arm, neck, or jaw, accompanied by dyspnea, diaphoresis, nausea, and apprehension [9][10][11]. However, up to 20–25% of infarctions are "silent" or asymptomatic, particularly in patients with diabetic autonomic neuropathy [9][10].
Acute heart failure (AHF) frequently complicates the course of AMI and represents a critical determinant of prognosis. Heart failure (HF) is defined as a clinical syndrome characterized by dyspnea, fatigue, swelling, and/or decreased exercise capacity resulting from structural or functional cardiac abnormalities that impair ventricular filling or ejection [7]. In the setting of AMI, AHF may arise de novo or as acute decompensation of chronic HF, with phenotypes ranging from pulmonary congestion to cardiogenic shock (CS) [1]. The pathophysiological paradigm of CS involves a myocardial ischemic insult leading to reduced contractile mass, decreased cardiac output, systemic hypoperfusion, and reflexive sympathetic/neurohormonal activation [6]. The Killip classification provides a rapid bedside tool for stratifying hemodynamic severity: Class I (no signs of HF), Class II (pulmonary congestion with rales), Class III (acute pulmonary edema), and Class IV (cardiogenic shock) [8]. Among AMI survivors, approximately 3.8% require HF admission within 12 months, with independent risk factors including older age, female sex, Killip class ≥2 on admission, and reduced left ventricular ejection fraction [3]. Despite advances in chronic HF management, outcomes in AHF remain poor, with 1-year mortality rates ranging from 25% for acute decompensated HF to 50% for those presenting with CS [1].
**The following diagram illustrates the mechanical complications of myocardial infarction that can precipitate or exacerbate acute heart failure:**
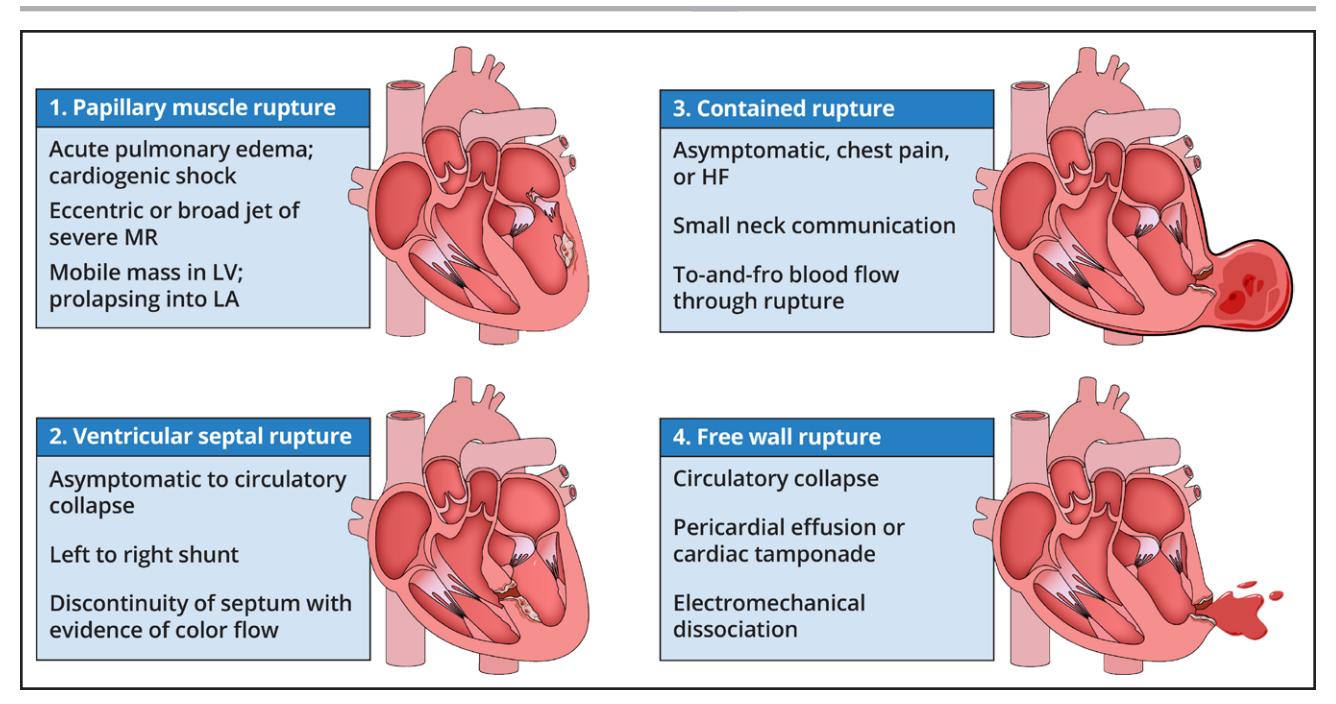
*Figure: Illustration of four critical mechanical complications of myocardial infarction—papillary muscle rupture, ventricular septal rupture, contained rupture, and free wall rupture—each of which can lead to acute hemodynamic deterioration and heart failure*
---
*This content is synthesized from retrieved literature for clinical reference. Please verify against original sources and apply individual patient judgment in clinical decision-making.*