Osteoporosis Medication Jaw Necrosis
A patient with osteoporosis developed medication-related osteonecrosis of the jaw following sequential treatment with denosumab and alendronate sodium. After undergoing a bisphosphonate holiday, how should the choice of medication be determined for restarting anti-osteoporosis therapy?
**For patients with a history of MRONJ who require resumption of anti-osteoporosis therapy after a drug holiday, teriparatide or raloxifene are recommended as alternative options, while resumption of antiresorptive agents (bisphosphonates, denosumab) is not absolutely contraindicated but requires shared decision-making after complete healing of MRONJ.**
---
## Clinical Evidence & Efficacy
### Alternative Agents After MRONJ
According to the 2024 OSHK Guideline for Clinical Management of Postmenopausal Osteoporosis in Hong Kong, the following principles apply for subsequent management after MRONJ[8]:
- **Teriparatide or raloxifene** may serve as alternative options after MRONJ[8].
- A history of MRONJ is **not an absolute contraindication** for resumption of antiresorptive drugs in patients with high fracture risk after **complete healing** of MRONJ[8].
- In clinical practice, both patients and clinicians are usually hesitant to resume antiresorptive therapy after MRONJ[8].
The Asia-Pacific consensus on long-term and sequential therapy for osteoporosis similarly states that selective estrogen receptor modulators (SERMs) can be considered treatment options for patients who have developed MRONJ instead of stopping anti-osteoporosis medications entirely[9].
### Resumption of Antiresorptive Therapy
The AAOMS (American Association of Oral and Maxillofacial Surgeons) advocates prioritization and support of continued bone health and the prevention of fragility fractures, emphasizing that the benefits of fracture prevention offered by antiresorptive therapy far exceed the risk of MRONJ[8].
---
## Treatment Selection Factors
### Patient-Specific Considerations
| Factor | Consideration |
|--------|---------------|
| **Fracture risk** | High fracture risk patients may still benefit from antiresorptive therapy after MRONJ healing |
| **MRONJ healing status** | Complete healing must be confirmed before considering resumption of antiresorptive agents |
| **Patient preference** | Shared decision-making is critical given the psychological impact of MRONJ |
| **Alternative options** | Teriparatide (anabolic) or raloxifene (SERM) offer non-antiresorptive pathways |
### Drug-Specific Considerations
- **Teriparatide**: An anabolic agent that stimulates bone formation rather than suppressing bone turnover, theoretically avoiding the mechanism implicated in MRONJ pathogenesis.
- **Raloxifene**: A SERM with a different mechanism of action (estrogen receptor agonist on bone) that does not carry the same MRONJ risk profile as bisphosphonates or denosumab[5].
- **Bisphosphonates/Denosumab**: Resumption is possible only after complete MRONJ healing and with careful benefit-risk assessment[8].
---
## Guideline Recommendations
| Source | Recommendation | Grade |
|--------|---------------|-------|
| 2024 OSHK Guideline (Hong Kong) | Teriparatide or raloxifene as alternative options after MRONJ | Expert opinion |
| 2024 OSHK Guideline (Hong Kong) | History of MRONJ is not an absolute contraindication for resumption of antiresorptive drugs after complete healing | Expert opinion |
| Asia-Pacific Consensus | SERMs can be considered for patients who developed MRONJ instead of stopping anti-osteoporosis medications | Consensus |
---
## Clinical Decision Pathway
**The following flowchart illustrates the drug selection and switching strategies for osteoporosis based on specific patient scenarios, including medication-related complications:**
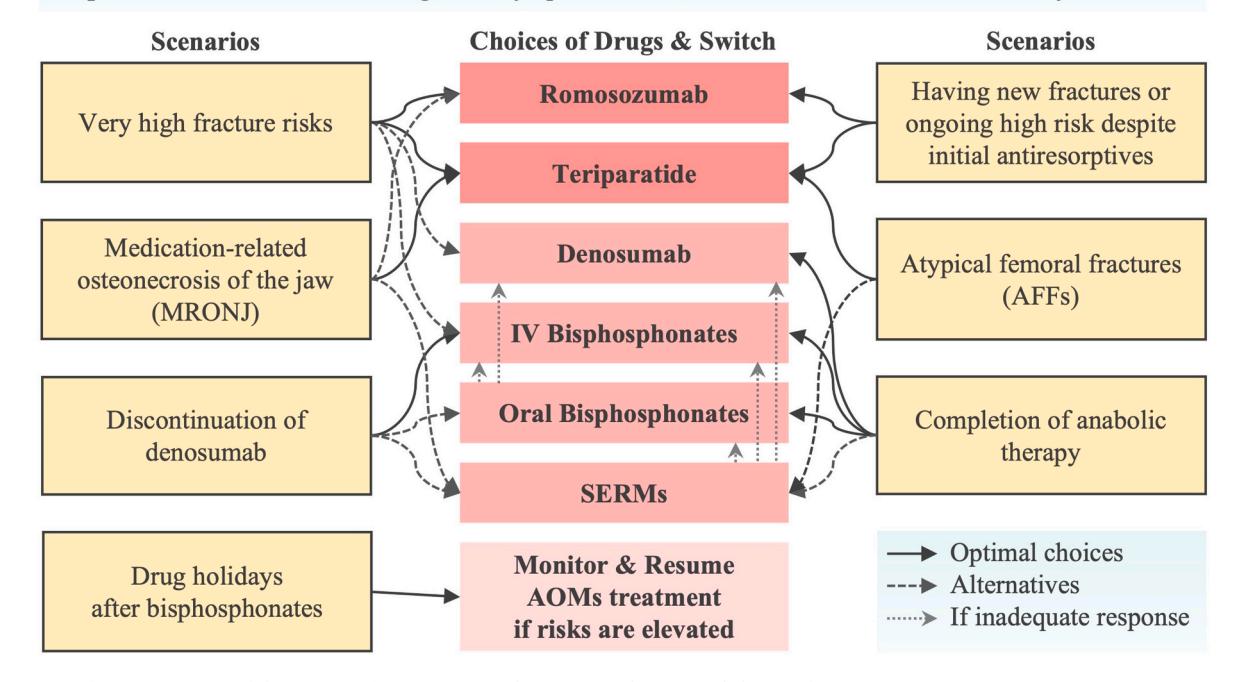
*Figure: A clinical flowchart detailing drug selection and switching strategies for osteoporosis based on specific patient scenarios, including high fracture risk and medication-related complications.*
---
## Critical Gaps
The current evidence does not provide specific guidance on:
- The optimal duration of drug holiday before considering resumption of therapy after MRONJ
- Head-to-head comparisons of teriparatide versus raloxifene specifically in the post-MRONJ population
- Long-term outcomes data for patients who resume antiresorptive therapy after MRONJ healing
---
## Conclusion
After MRONJ in a patient with prior sequential denosumab and alendronate therapy, teriparatide or raloxifene are the preferred alternative agents; resumption of antiresorptive therapy is possible only after complete MRONJ healing and with careful shared decision-making weighing fracture prevention benefits against the risk of recurrence.
---
*Disclaimer: This analysis is based on retrieved clinical guidelines and consensus statements. Clinical decisions should be individualized based on the patient's fracture risk profile, MRONJ healing status, and preferences, with verification against current local prescribing information.*