Mechanical Thrombectomy vs Thrombolysis
What evidence compares mechanical thrombectomy versus intravenous thrombolysis in cardioembolic stroke?
Based on the retrieved evidence, the primary comparison in the literature is between **mechanical thrombectomy (MT) alone** versus **bridging therapy (intravenous thrombolysis [IVT] followed by MT)** in patients with acute ischemic stroke (AIS) due to large vessel occlusion (LVO), rather than a direct comparison of MT versus IVT as standalone treatments. The evidence does not specifically isolate a "cardioembolic" etiology subgroup for this comparison.
### Clinical Evidence & Efficacy
The available evidence focuses on whether IVT provides additional benefit before MT in eligible patients.
**1. Guideline Recommendations (Strongly Favor Bridging Therapy)**
The **European Stroke Organisation (ESO)-ESMINT expedited recommendation** provides a strong directive for patients with anterior circulation LVO who are eligible for both treatments [5].
- **For patients directly admitted to a thrombectomy-capable center (≤4.5 hours of symptom onset):** IVT plus MT is **recommended** over MT alone. Quality of evidence: Moderate. Strength of recommendation: Strong [5].
- **For patients admitted to a non-thrombectomy-capable center (≤4.5 hours):** IVT followed by rapid transfer to a thrombectomy center is **recommended** over omitting IVT. Quality of evidence: Low. Strength of recommendation: Strong [5].
- **For wake-up stroke patients (≤4.5 hours of recognition) with LVO:** IVT plus MT is **suggested** over MT alone in selected patients meeting specific imaging criteria (e.g., DWI-FLAIR mismatch or perfusion mismatch) [5].
**2. Meta-Analysis Evidence (Mixed Results)**
A systematic review and meta-analysis by Zheng et al. (search up to June 2022) compared MT+IVT versus MT alone [2]. The findings are nuanced:
- **Functional Independence (mRS 0-2):** The meta-analysis showed a statistically significant benefit for the bridging therapy (MT+IVT) group.
- **Successful Recanalization (SR):** Bridging therapy was associated with higher rates of successful recanalization.
- **Mortality:** Bridging therapy was associated with lower three-month mortality.
- **Safety (Intracranial Hemorrhage):** The incidence of any intracerebral hemorrhage (aICH) was higher in the bridging therapy group, though symptomatic ICH (sICH) rates were comparable.
**The following forest plot illustrates the meta-analysis results comparing MT+IVT versus MT alone:**
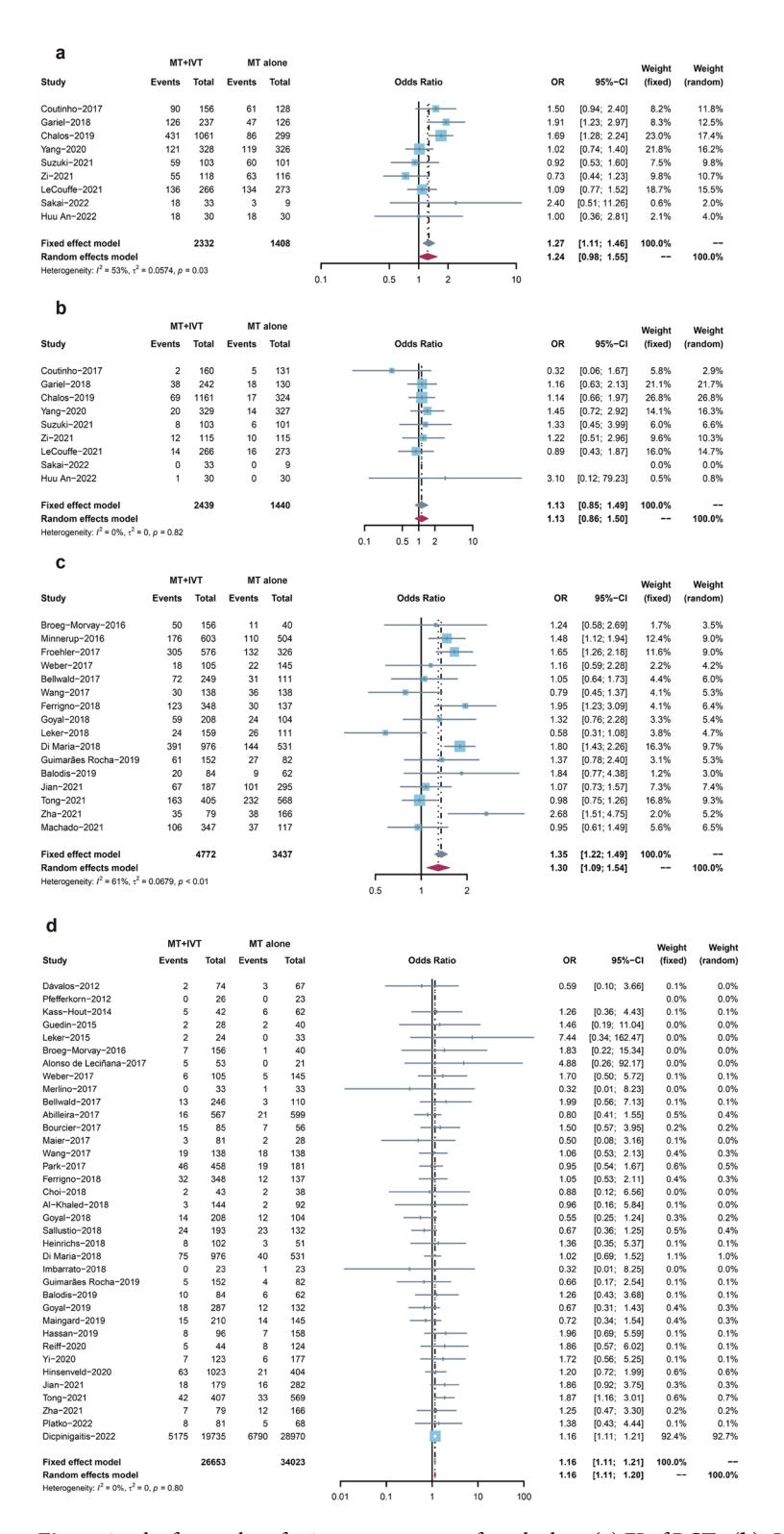
*Figure: Forest plots (a-d) showing meta-analysis results for functional independence, excellent outcomes, successful recanalization, and symptomatic intracerebral hemorrhage for MT+IVT vs. MT alone [2].*
**3. Recent RCT and Propensity-Matched Data (No Significant Difference)**
More recent evidence challenges the meta-analysis findings, suggesting non-inferiority of MT alone.
- **DIRECT-MT and SKIP Trials:** The retrieved context notes that two studies in Asian regions showed non-inferiority of MT alone compared to bridging therapy, while three studies in other populations did not, leading to overall uncertainty [4].
- **DMVO Study (Propensity-Matched):** A multinational multicenter study specifically focused on **distal medium vessel occlusion (DMVO)** found no significant difference between MT+IVT and IVT alone [1].
- **Functional Independence (mRS 0-1):** Adjusted OR 1.21 (95% CI 0.81-1.79; P=0.35) [1].
- **Mortality at 90 days:** OR 0.75 (95% CI 0.44-1.29; P=0.30) [1].
- **Safety:** Any intracranial hemorrhage was significantly higher in the MT+IVT group (OR 0.43, 95% CI 0.29-0.64) [1].
**The following forest plots from a meta-analysis of RCTs show no significant difference in outcomes between direct MT and bridging therapy:**
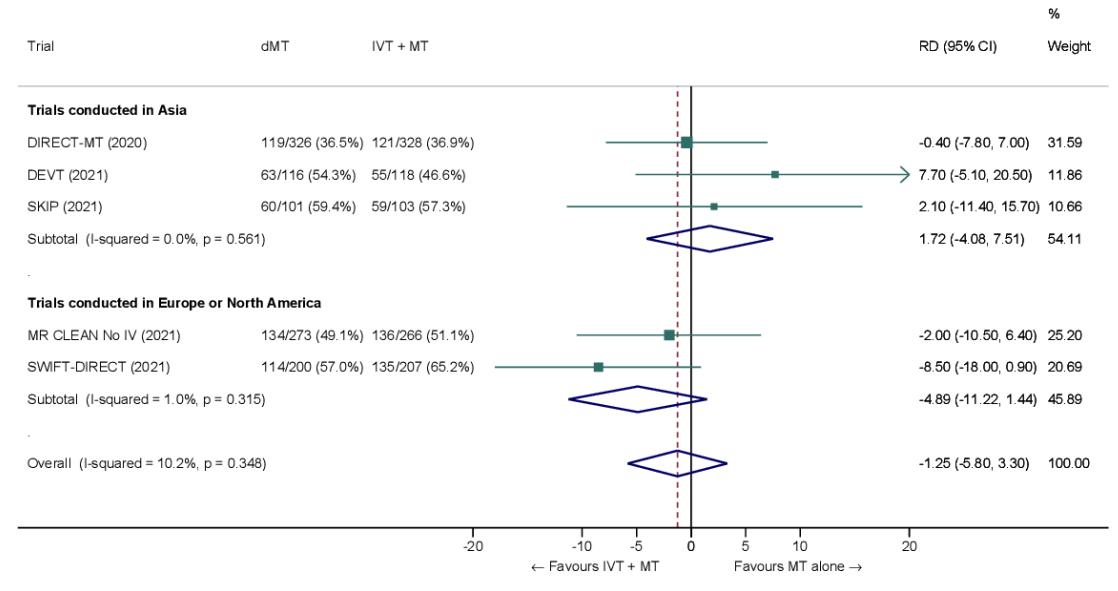
*Figure: Forest plot showing the comparison of direct MT vs. bridging therapy for the outcome of functional independence (mRS 0-2) at 90 days [4].*
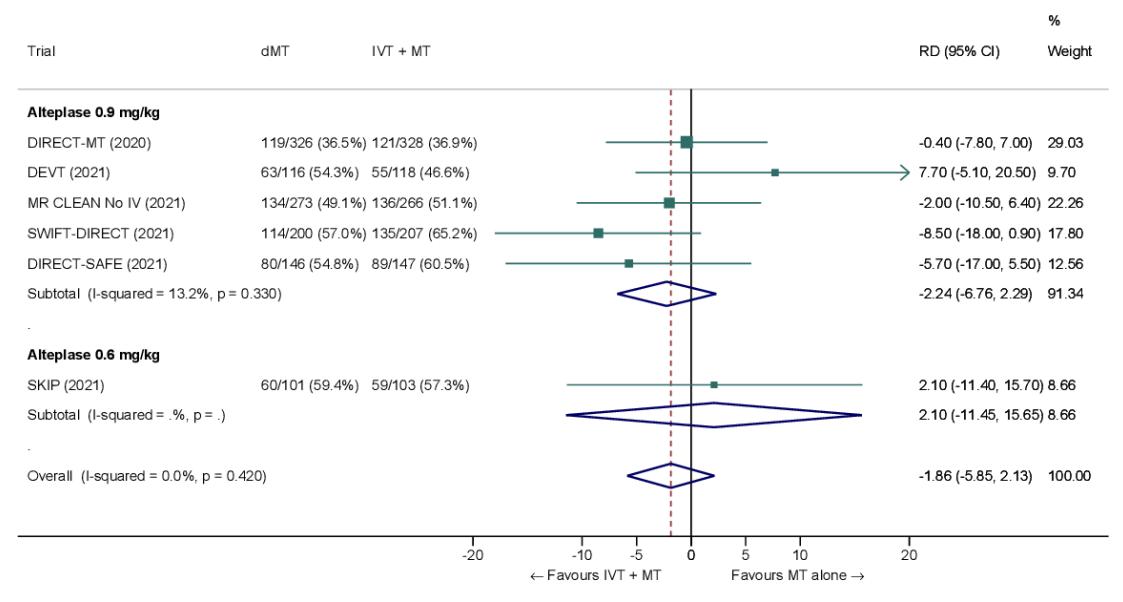
*Figure: Forest plot showing the comparison of direct MT vs. bridging therapy for the outcome of mortality at 90 days [4].*
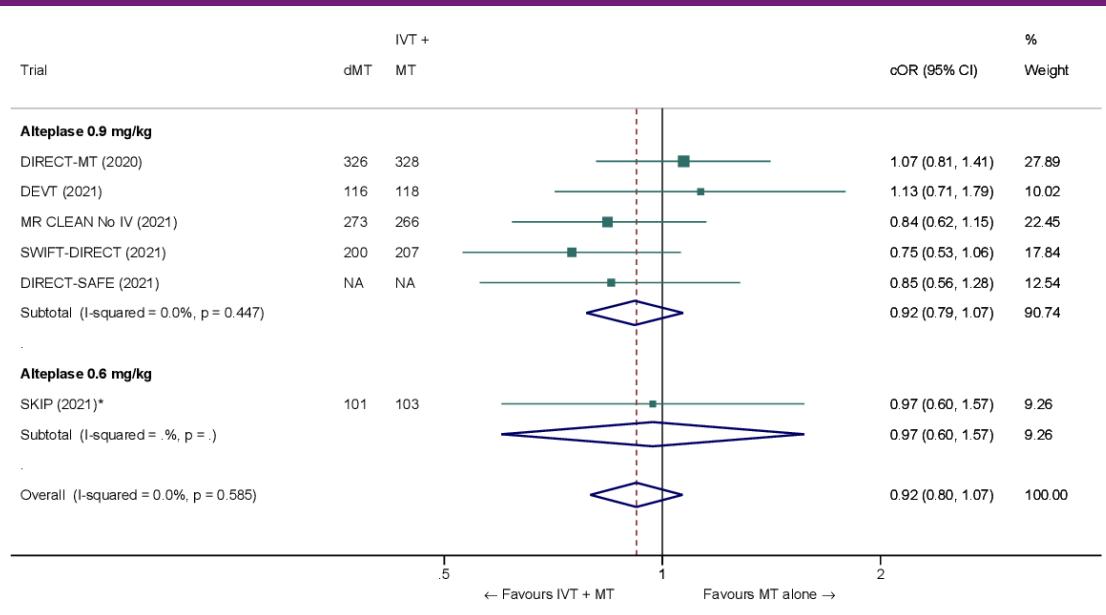
*Figure: Forest plot showing the comparison of direct MT vs. bridging therapy for the outcome of symptomatic intracerebral hemorrhage (sICH) [4].*
### Critical Gaps
- **Cardioembolic Subgroup:** The retrieved evidence does not provide a dedicated subgroup analysis for cardioembolic stroke. The efficacy and safety of MT alone vs. bridging therapy may differ in this population due to the nature of the embolic clot (e.g., fibrin-rich vs. platelet-rich), but this is not addressed in the provided context.
- **Distal Medium Vessel Occlusion (DMVO):** The evidence for DMVO is limited to a single propensity-matched study [1], and the optimal strategy remains uncertain. The ESO guidelines [5] are specific to anterior circulation LVO.
### Conclusion
Current evidence is conflicting: strong guideline recommendations from ESO-ESMINT favor bridging therapy (IVT+MT) for eligible LVO patients, while recent RCTs and meta-analyses show non-inferiority of MT alone with a potential safety advantage (lower any ICH). The evidence does not specifically address the cardioembolic stroke subpopulation.
---
*This analysis is based on retrieved literature and is intended for clinical reference. Clinical decisions should be made based on individual patient characteristics, local protocols, and the most current guidelines.*