COPD Treatment Elderly
What treatment strategies are recommended for elderly patients with COPD?
For elderly patients with COPD, the recommended treatment strategy is a **stepwise, individualized approach** that prioritizes symptom control, exacerbation prevention, and mortality reduction, with critical modifications for age-related physiological changes, polypharmacy, and multimorbidity.
---
## Clinical Evidence & Efficacy
### Pharmacotherapy: Step-Up Approach Based on GOLD 2026
The cornerstone of management is a stepwise escalation of pharmacotherapy guided by symptom burden (mMRC or CAT) and exacerbation risk, as outlined in the GOLD 2026 report and the 2023 Canadian Thoracic Society (CTS) Guideline [1][6].
**The following algorithm illustrates the stepwise escalation of therapeutic interventions based on disease severity:**
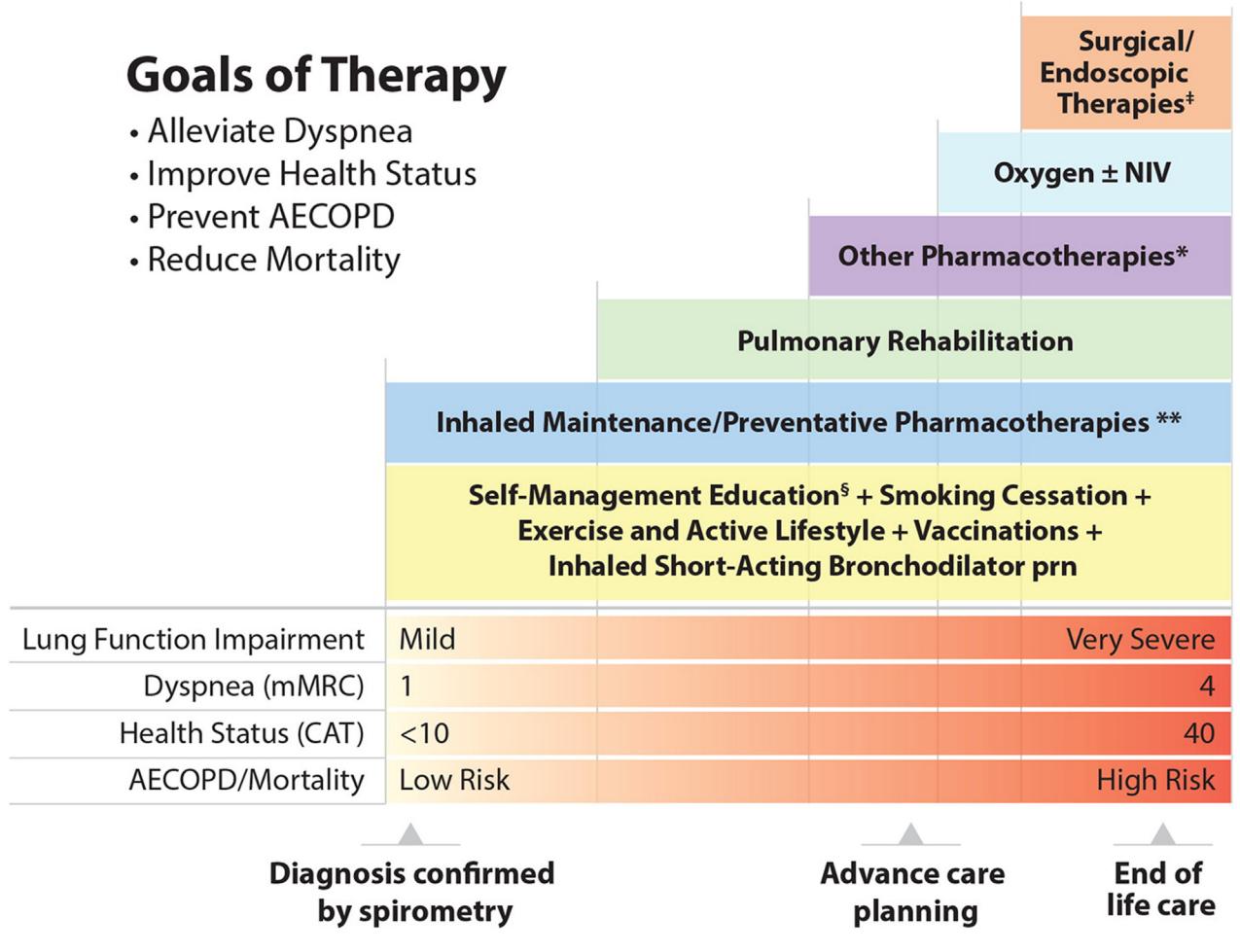
*Figure: A stepped management algorithm for COPD illustrating the escalation of therapeutic interventions based on increasing disease severity, symptoms, and exacerbation risk.*
**The following flowchart details the pharmacological treatment pathways based on symptoms and blood eosinophil counts:**
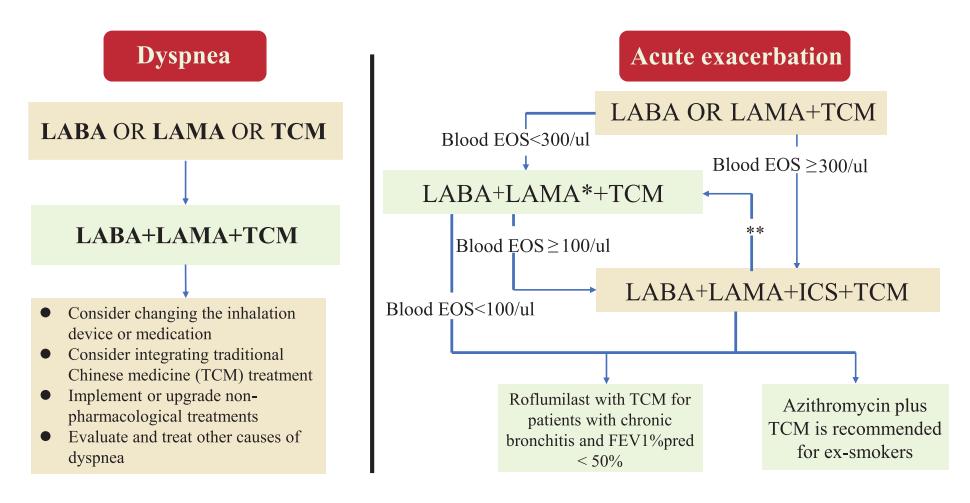
*Figure: This flowchart outlines pharmacological treatment pathways for COPD patients based on symptoms of dyspnea or acute exacerbations, incorporating blood eosinophil counts and Traditional Chinese Medicine considerations.*
**The following flowchart details the escalation of pharmacological therapy based on CAT/mMRC scores, FEV1 percentages, and AECOPD risk levels:**
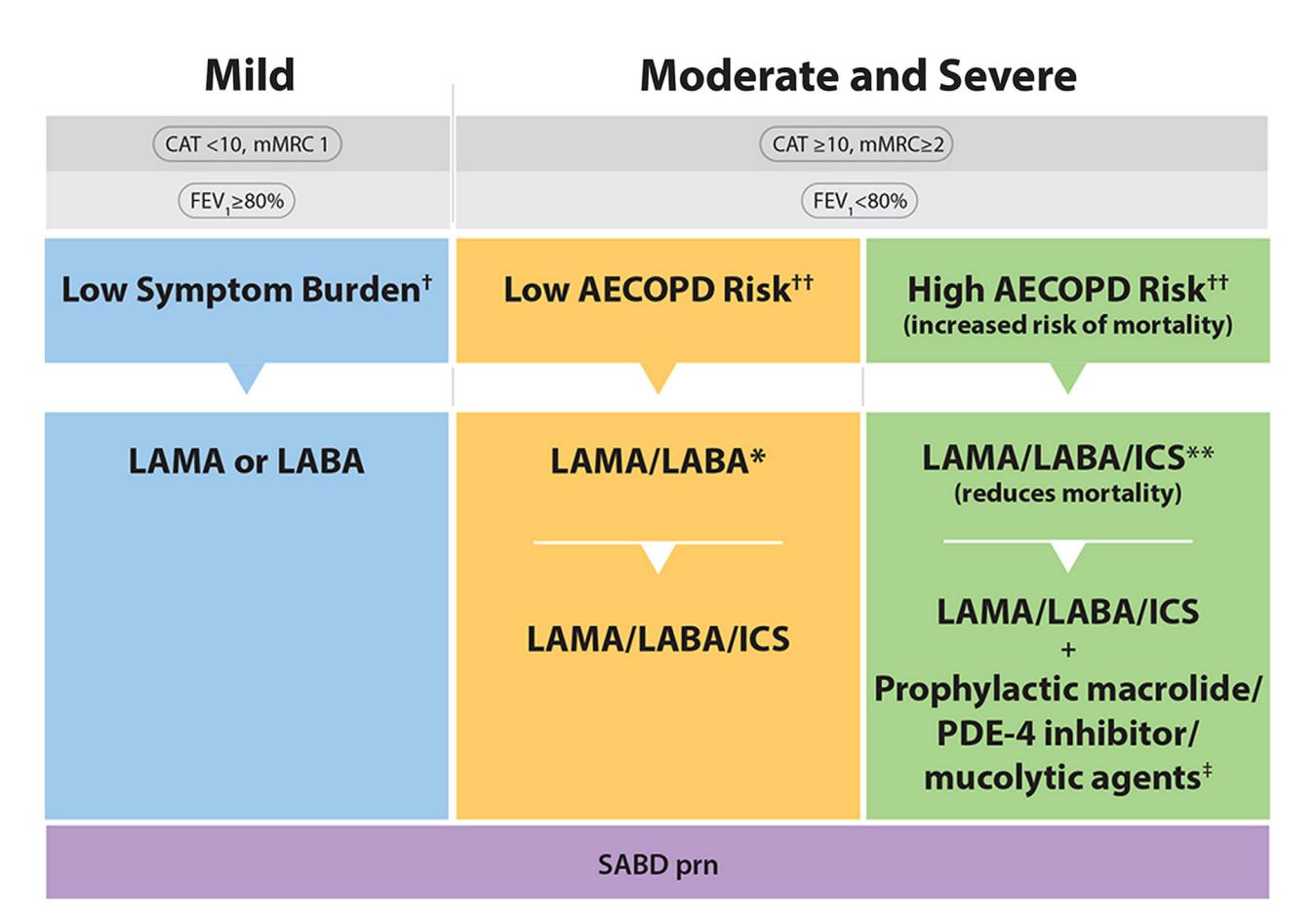
*Figure: A clinical flowchart detailing the escalation of COPD pharmacological therapy based on CAT/mMRC scores, FEV1 percentages, and AECOPD risk levels.*
**Key Pharmacotherapy Recommendations:**
- **Initial Therapy**: Long-acting bronchodilator (LABD) maintenance therapy is recommended for all symptomatic patients with spirometry-confirmed COPD [6].
- **Dual Therapy**: For patients with moderate-to-severe dyspnea and/or poor health status, single-inhaler dual therapy (LAMA/LABA or ICS/LABA) is recommended [6].
- **Triple Therapy**: For patients with persistent moderate-to-severe dyspnea and/or poor health status despite dual therapy, or those at high risk of acute exacerbations (AECOPD), single-inhaler triple therapy (SITT) is recommended. The 2023 CTS guideline specifically suggests SITT in all patients at high risk of AECOPD, as it reduces mortality in individuals with moderate-severe disease [6].
### Exacerbation Management in the Elderly
Elderly patients are particularly vulnerable to exacerbations, which are typically triggered by infections [8].
- **Antibiotic Therapy**: Must be initiated promptly on suspicion of infection, covering a broad spectrum of pathogens. Hospitalization is mandatory for elderly patients with COPD exacerbations [8].
- **Choice of Antibiotics**: Should reflect the acquisition setting (community vs. nosocomial) and local resistance patterns. Fluoroquinolones are noted to be particularly toxic for the elderly brain, potentially inducing delirium. Beta-lactam antibiotics (e.g., amoxicillin/clavulanate) or macrolides (e.g., clarithromycin) are considered safer if dosed correctly for renal/hepatic function [8].
- **Corticosteroids**: Oral high-dose glucocorticoids (prednisolone 30-40 mg/day for 7-10 days) are a successful therapeutic supplement for exacerbations [8].
- **Mucolytics and Antitussives**: Mucolytics (e.g., acetylcysteine) lack proven efficacy and may cause side effects. Antitussives are not recommended, as coughing is important to prevent pneumonia in the elderly [8].
### Palliative and Supportive Care
Palliative care is essential for all stages of COPD, not just end-of-life. The GOLD 2026 report emphasizes that even with optimal medical therapy, many patients experience distressing breathlessness, fatigue, anxiety, and depression [1]. Early access to palliative care can improve quality of life and even survival [4]. Key components include symptom control (dyspnea, fatigue, depression, anxiety, insomnia), advance care planning, and discussions about resuscitation preferences and place of death [1][4].
---
## Dosing & Administration
### Geriatric-Specific Modifications
- **Start Low, Go Slow**: While specific dosing protocols for elderly patients are not detailed in the retrieved context, the principle of starting at lower doses and titrating gradually is a standard geriatric precaution.
- **Renal and Hepatic Function**: Dosing of all medications, especially antibiotics, must be strictly adapted to altered pharmacokinetics in the elderly, primarily related to kidney and liver function [8].
- **Inhaler Technique**: Proper inhaler technique is of high relevance. Techniques should be demonstrated and confirmed using the teach-back approach at every visit to ensure adherence and correct use [7].
---
## Safety Profile
### Key Contraindications and Precautions
- **Cardiac Comorbidity**: COPD in the elderly frequently coexists with coronary heart disease and heart failure (about 20% of cases) [8]. Bronchodilators (beta-agonists, theophylline) can stress the heart, creating relative contraindications. An exact differential diagnosis between COPD and heart failure is critical, as beta-blockers (indicated for heart failure) may be contraindicated in obstructive lung disease [8].
- **Benzodiazepines**: Caution is warranted due to potential depressive effects on respiratory drive and inherent risks in the elderly of dependence, cognitive impairment, and falls [4].
- **Antibiotic-Associated Diarrhea**: In elderly patients, this can rapidly induce dehydration, electrolyte disorders, and venous thromboses, requiring aggressive rehydration and electrolyte substitution [8].
### Drug Interactions
- **Polypharmacy**: Elderly COPD patients often have multiple comorbidities (25% have two additional diagnoses, 17% have three) [8]. A thorough review of all medications is mandatory to avoid drug-drug interactions.
---
## Guideline Recommendations
| Recommendation | Source | Strength |
|---|---|---|
| LABD maintenance therapy for all symptomatic patients | 2023 CTS Guideline [6] | Strong |
| Single-inhaler dual therapy for moderate-to-severe dyspnea | 2023 CTS Guideline [6] | Strong |
| Single-inhaler triple therapy for high AECOPD risk | 2023 CTS Guideline [6] | Strong (reduces mortality) |
| Early palliative care for persisting symptoms | GOLD 2026 [1], COPD-X Plan [4] | Strong |
| Smoking cessation as most important intervention | Geriatric Practice [7] | Strong |
| Vaccinations (influenza, pneumococcus, RSV, COVID-19) | Multidisciplinary Consensus [2] | Strong |
---
## Critical Gaps in Current Evidence
- **Specific Geriatric Dosing Protocols**: The retrieved evidence does not provide specific dose adjustment tables for elderly patients for most COPD medications. The GOLD 2026 report itself notes that no separate chapters are devoted to elderly patients [1][8].
- **Efficacy of Antidepressants**: A 2018 Cochrane review concluded there is insufficient evidence to make recommendations on the use of SSRIs for depression in COPD patients [4].
---
## Conclusion
The recommended treatment strategy for elderly patients with COPD is a stepwise, individualized pharmacotherapy approach (LABD → dual therapy → triple therapy) guided by symptom burden and exacerbation risk, combined with early palliative care, aggressive exacerbation management with careful antibiotic selection, and mandatory consideration of age-related physiological changes and cardiac comorbidities.
---
*This response is based on retrieved clinical guidelines and literature. All clinical decisions should be verified against the latest prescribing information and tailored to the individual patient's comorbidities, organ function, and preferences.*