Dual Antiplatelet Therapy
A patient on long-term dual antiplatelet therapy (aspirin plus clopidogrel) is scheduled to undergo laparoscopic cholecystectomy. Regarding the preoperative bridging strategy, is it currently recommended to use low molecular weight heparin, or is it suggested that bridging be omitted due to the low risk of thrombosis? Please provide the recommendations from the latest ACCP antithrombotic guidelines.
**Conclusion**: For a patient on dual antiplatelet therapy (DAPT) undergoing laparoscopic cholecystectomy, the 2022 ACCP guidelines do **not** recommend LMWH bridging for antiplatelet agents. The perioperative strategy focuses on timing of antiplatelet cessation and resumption based on thrombotic risk, not on bridging with an anticoagulant.
---
## Perioperative Management of Antiplatelet Therapy: ACCP 2022 Guideline Recommendations
### 1. Core Principle: No Bridging for Antiplatelet Agents
The 2022 American College of Chest Physicians (ACCP) Clinical Practice Guideline on the Perioperative Management of Antithrombotic Therapy explicitly addresses the management of patients on antiplatelet drugs [2][3]. **LMWH bridging is a strategy reserved for patients on vitamin K antagonists (e.g., warfarin) who are at high thromboembolic risk** [1][2]. For patients on antiplatelet therapy (aspirin, P2Y12 inhibitors, or DAPT), the guideline does **not** recommend the use of heparin bridging. The perioperative approach instead centers on:
- **Risk stratification** of perioperative bleeding vs. thrombotic risk
- **Timing of drug cessation** prior to surgery
- **Timing of drug resumption** postoperatively
### 2. Recommended Cessation and Resumption Timelines
**Aspirin**:
- **Minor procedures** (dental, dermatologic, cataract): May be continued [1].
- **Major noncardiac surgery** (e.g., laparoscopic cholecystectomy): Withhold for **≥7 days** before surgery [1].
**Clopidogrel (P2Y12 inhibitor)**:
- **Elective surgery**: Discontinue **5–7 days** prior to surgery [1][2].
- **High-bleeding-risk surgery** (intracranial, ocular, or high-bleeding-risk procedures): Typically suspend [1].
**Postoperative resumption**:
- Hemostasis must be achieved before restarting antiplatelet agents [1].
- Resumption timing is individualized based on bleeding risk and thrombotic risk.
### 3. Special Considerations for DAPT and Stent-Related Thrombotic Risk
The ACCP guideline emphasizes that elective surgery should be deferred:
- **≥6 weeks** after bare-metal stent (BMS) placement
- **≥6 months** after drug-eluting stent (DES) placement [1]
If surgery cannot be delayed within these windows, DAPT should be continued perioperatively [1]. After these periods, the P2Y12 inhibitor may be temporarily suspended for surgery while aspirin is often continued.
### 4. Visual Summary of Perioperative Antiplatelet Management
**The following timeline illustrates the perioperative management of antiplatelet therapy, including discontinuation of oral P2Y12 inhibitors and the use of Cangrelor as a bridging agent while continuing aspirin:**
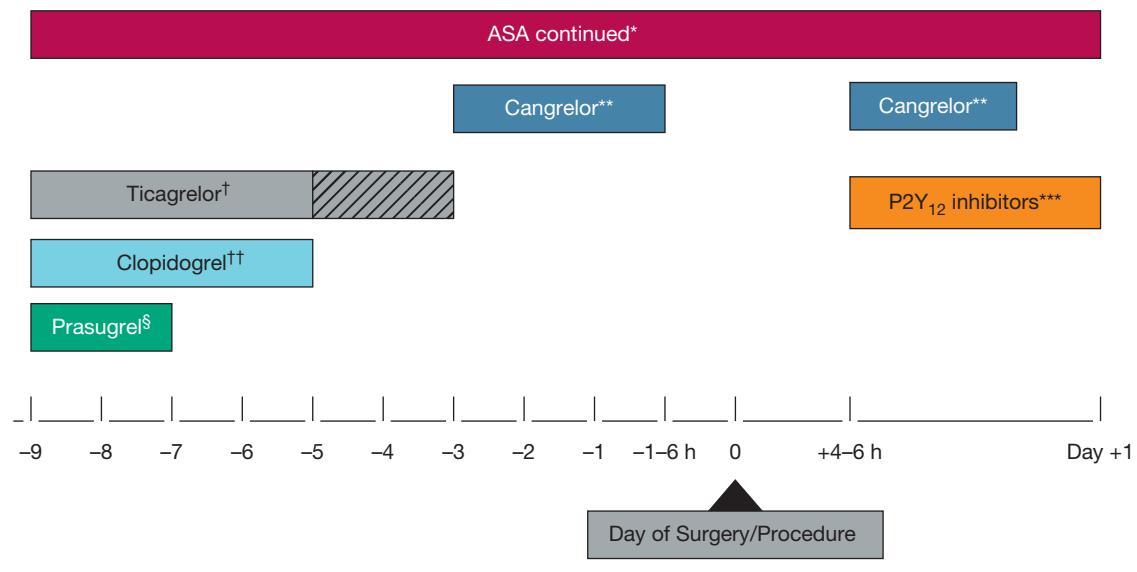
*Figure: Timeline for perioperative management of antiplatelet therapy, detailing the discontinuation of oral P2Y12 inhibitors and bridging with Cangrelor.*
**The following diagram outlines the perioperative management of Warfarin and LMWH bridging therapy based on surgical bleeding risk, specifying cessation and resumption timelines relative to the day of surgery:**
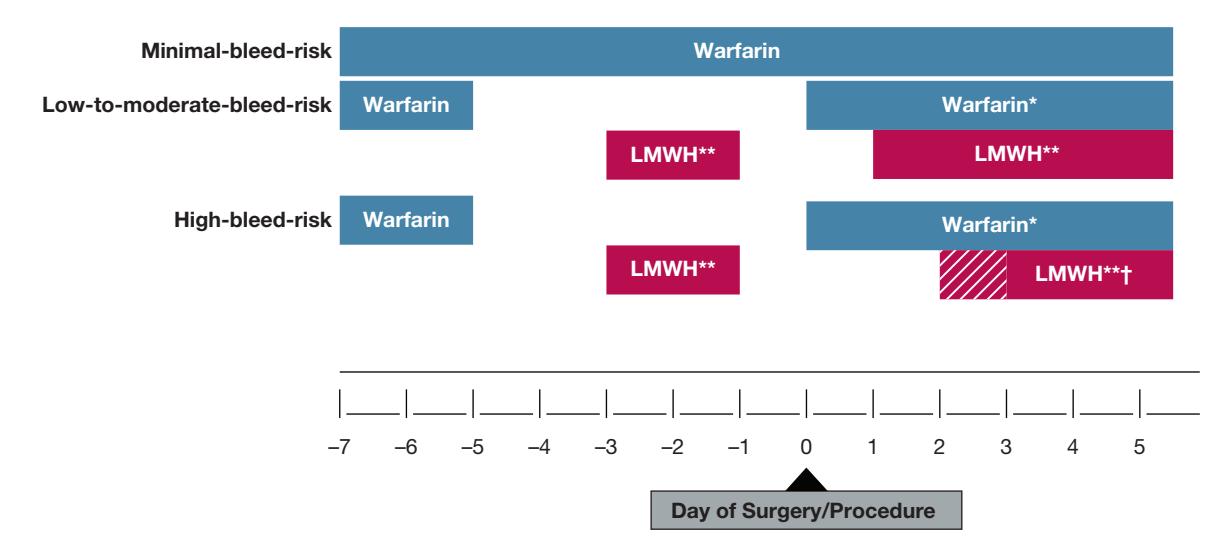
*Figure: This chart outlines the perioperative management of Warfarin and LMWH bridging therapy based on surgical bleeding risk, specifying cessation and resumption timelines relative to the day of surgery.*
### 5. Key Distinction: When Is Bridging Used?
| Therapy Type | Bridging Indication | Bridging Agent |
|---|---|---|
| **Warfarin (VKA)** | High thromboembolic risk (e.g., CHA₂DS₂-VASc ≥7, mechanical mitral valve, recent CVA/VTE ≤3 months) | Therapeutic-dose LMWH or UFH [1] |
| **DOACs** | Not routinely needed (predictable short half-life) | N/A [1] |
| **Antiplatelet (Aspirin, P2Y12i, DAPT)** | **Not recommended** | N/A [2] |
### 6. Clinical Application to This Case
For a patient on DAPT (aspirin + clopidogrel) undergoing laparoscopic cholecystectomy:
1. **Assess thrombotic risk**: Determine the indication for DAPT (e.g., recent stent, recent ACS, prior CVA). If within the high-risk post-stent window (BMS <6 weeks, DES <6 months), consider deferring elective surgery.
2. **Discontinue clopidogrel** 5–7 days preoperatively; **discontinue aspirin** ≥7 days preoperatively.
3. **Do NOT use LMWH bridging** — this is not indicated for antiplatelet therapy per ACCP guidelines.
4. **Resume antiplatelet therapy** postoperatively once hemostasis is confirmed.
---
### Further Diagnostic Suggestions (Reference Only)
To enable a more accurate assessment, if available, please consider providing:
- **Indication for DAPT**: Recent stent placement (type and date), recent ACS, or prior CVA — this determines whether surgery can proceed or should be deferred.
- **CHA₂DS₂-VASc score**: If the patient also has atrial fibrillation, this score informs bridging decisions for warfarin, but not for antiplatelet therapy.
---
*Disclaimer: This content is AI-generated based on retrieved literature and is intended for clinical reference only. Please verify all recommendations against the full guideline text and apply individual patient judgment.*